Histology of the Ear (G 7.78a, 7.78b)
I. Bony Labyrinth
Embedded within the petrous portion of the temporal bone is the bony labyrinth which consists of the central vestibule, three semicircular canals, which arise and end at the vestibule, and the cochlea. It contains a fluid called perilymph, which has a composition similar to extracellular fluids (high in Na+, low in K+).
- Between the vestibule and middle ear is a tissue-covered hole in the bone, the “oval window”. The footplate of the stapes [DigitalScope] is attached to the oval window on the middle ear side. Here, vibrations of the tympanic membrane are converted into fluid vibrations of perilymph via the bones of the middle ear.
- The cochlea [DigitalScope], located anteriomedially to the vestibule consists of a tube spiraling around a bony axis (the modiolus).
B. Vestibulocochlear Nerve - cochlear division and vestibular division - [slide EAR-2, DigitalScope]
The vestibulocochlear nerve (CN VIII) enters the petrous temporal bone to innervate the inner ear. The innervation of the cochlea and vestibule is as follows:
- The cell bodies of the cochlear neurons occupy a canal (the spiral canal) that spirals up the modiolus. This spiral aggregate of nerve cells is called the spiral (or cochlear) ganglion [DigitalScope]. These are bipolar sensory neurons: their dendrites synapse with the hair cells in the organ of Corti (discussed below) and their axons come together in the cochlear nerve, which occupies a central canal in the modiolus and exits at the base of the cochlea.
- In the sensory regions of the vestibule, hair cells of the maculae and cristae (discussed below) synapse with dendrites of a corresponding aggregation of sensory neurons in the vestibular (or Scarpa’s) ganglion [DigitalScope], which then send their axons through the vestibular nerve. The processes of the vestibular nerve join with those of the cochlear nerve to form the vestibulocochlear nerve (cranial nerve VIII)(orientation).
II. Membranous labyrinth - The membranous labyrinth consists of the interconnected utricle, saccule, three semicircular ducts, the endolymphatic duct and sac, and the cochlear duct. It contains a fluid, endolymph, much like intracellular fluid in composition (high K+, low Na+).
A. Otolith Organs - Macula of the Utricle and Saccule - [slide EAR-2, DigitalScope]
The utricle and the saccule contain the otolith organs that lie within the bony vestibule (orientation) and serve to detect linear acceleration. These otolith organs consist of sensory areas called maculae, and you should note that they are oriented somewhat perpendicular to each other to be able detect movement in different planes. Taking a closer look at a macula (example) [DigitalScope], you should be able to identify the sensory epithelium comprised of hair cells and supporting cells. It is overlaid by a gelatinous material (otolithic membrane) in which are embedded calcite crystals (otoliths or otoconia). The otoconia are quite visible in some slides, hardly visible in others. During linear acceleration, inertial drag of these crystals causes deflection of the hair cells and subsequent signaling into the CNS. Beneath the sensory epithelium is a delicate connective tissue (filled with perilymph) and nerve fibers from the bipolar neurons of the vestibular (Scarpa’s) ganglion.
B. Semicircular Canals and Cristae Ampullari - [slide EAR-4, DigitalScope]
The semicircular ducts have dilations (ampullae) near their origins from the utricle. Each ampulla has a ridge of tissue, or crista ampullaris, (example) [DigitalScope] that projects into the lumen. The crista has a sensory epithelium similar to that of the macula; recall, however, that the cristae are specialized to detect angular (or rotational) acceleration. The hairs of the hair cells project into a gelatinous material called the cupula. The cupula projects into the lumen more than the otolithic membrane of the macula, and lacks otoconia. Here, inertial drag of the perilymph pushes on the cupula and causes deflection of the hair cells and subsequent signaling into the CNS.
What would happen if any otoconia or other debris were to become lodged somewhere in a semicircular canal or in a cupula? Answer
Note that the “membrane” of the membranous labyrinth is suspended from the bone by a delicate connective tissue and that in the Ear-1 and Ear-2 slides this tissue has torn such that the membrane is now squished up against the crista, so there’s not much of the cupula that can be seen.(orientation)
C. Cochlear Duct and Organ of Corti
[slide EAR-1, DigitalScope]
[slide 80a, DigitalScope]
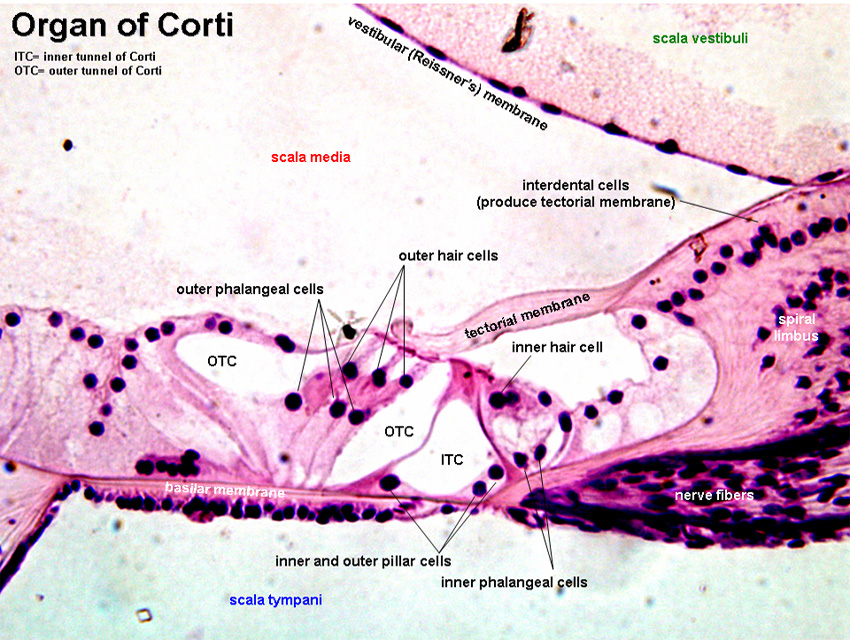
The cochlear duct [DigitalScope] or scala mediacontains the organ of Corti, which detects sound (hearing). The cochlear duct is a triangular tube that is suspended in the middle of the spiraling bony labyrinth of the cochlea, thus subdividing this space into three spiraling sub-compartments, or “scalae”: the scala vestibuli, which opens on the vestibule; the scala media; and the scala tympani, which ends at the round window (the round window is not seen in any your slides). The scala vestibuli and scala tympani are both elements of the bony labyrinth and contain perilymph; the scala media or cochlear duct is an element of the membranous labyrinth and contains endolymph.
Elements of the cochlear duct that can be seen in cross section are: (orientation)
- The vestibular membrane (also called Reissner’s membrane) is the tissue separating the cochlear duct from the scala vestibuli.
- The stria vascularis (example) [DigitalScope] is a stratified epithelium along the outer wall of the cochlear duct that is unique in that it is vascularized (most epithelia are avascular) by an extensive capillary network. Cells of the stria vascularis are responsible for the production and maintenance of endolymph.
- The basilar membrane [DigitalScope] extends from the tip of the osseous spiral lamina of the central modiolus to the outer wall of the cochlea and separates the cochlear duct from the scala tympani. The organ of Corti rests on the basilar membrane. Notice that the width of the basilar membrane changes such that it is shorter at the base and longer toward the apex of the cochlea. What is the significance of this change in length?
- The organ of Corti [DigitalScope] consists of two kinds of hair cells and various supporting cells in a complex arrangement.
The organ of Corti contains: (orientation)
- The outer hair cells surrounded by outer phalangeal cells. There are three rows of outer hair cells. The apices of these cells and their phalangeal cells are joined together to form the reticular membrane (also called reticular lamina or apical cuticular plate) that separates endolymph in the scala media from underlying corticolymph and perilymph of the scala tympani. Lateral to the outer hair cells and phalangeal cells are other support cells, but you don’t need to worry about knowing their specific types. Note that outer hair cells account for only ~5-10% of the sensory input into the auditory system. The primary function of outer hair cells is actually to contract when stimulated, thus “pulling” on the tectoral membrane thereby stimulating the inner hair cells (see animation).
- Outer and inner pillar cells outline a triangular shaped tunnel, called the inner tunnel, which is filled with perilymph-like fluid called corticolymph.
- The inner hair cells are in a single row close to the inner pillar cells (you may see more than one inner cell nucleus because of the thickness of the section). Note that the inner hair cells account for ~90-95% of the sensory input into the auditory system.
- The organ of Corti is overlaid by a gelatinous tectorial membrane (produced and maintained by the columnar cells found atop the spiral limbus just medial to the organ of Corti).
- Nerve fibers enter the organ of Corti through openings in a shelf of bone extending from the modiolus like the thread of a screw. The nerve fibers pass between supporting cells to synapse with the hair cells. Compare the innervation and function of the inner vs. outer hair cells.
A few notes about deafness: Disruption of any part of the process by which sound waves are transduced into input into the auditory portion of the CNS will result in “deafness.” Damage to the eardrum or ossicles results in so-called “conduction” deafness whereby sound waves are no longer transmitted into the inner ear. In this instance, a patient would NOT be able to hear a tuning fork held near the pinna, and the loss of hearing would extend across the entire range of frequencies. However, placing the stem of the fork on a bony part of the skull (e.g. the mastoid process) would then transmit vibrations directly to the inner ear (via the bone) where they could then be “heard.”
Loss of components within the cochlea results in sensorineural deafness which is more frequency-specific (i.e. the patient will not be able to hear specific pitches depending on the location of the damage in the cochlea). Loss of OUTER HAIR CELLS in a particular region of the cochlea would result in a “threshold shift” whereby sound of a particular frequency could still be detected (because the inner hair cells are still intact), but it would have to be LOUDER to make up for the fact that there are no outer hair cells to help stimulate the inner hair cells. This type of hearing loss can be compensated by a hearing aid.
Loss of INNER HAIR CELLS in a particular region of the cochlea would result in an almost complete inability to detect specific frequencies regardless of how loud they are. Loss of SPIRAL GANGLION CELLS would have a similar effect since these are the cells that actually project into the CNS. In both cases, the deafness could only be corrected with a cochlear implant.
|
{kind=link}